Pituitary Gland: Structure, Secretions, Hormones, Functions and Disorders
The pituitary gland is a small, reddish‑gray, endocrine organ located at the base of the brain, just behind the optic chiasma, as an extension of the hypothalamus. The average weight of the pituitary gland in gm is about 0.5–0.6 g in females and 0.6–0.7 g in males. Because it secretes many hormones that regulate growth, metabolism, reproduction, and stress responses, it is often called the “master gland” of the endocrine system.

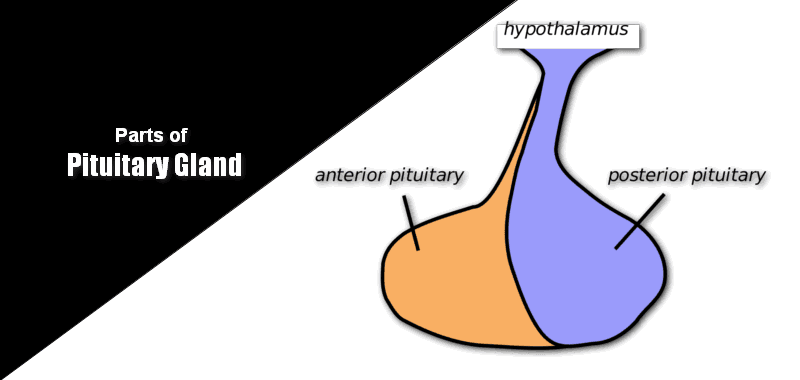
What are the basic parts of Pituitary Gland?
Anatomically, the pituitary gland is divided into three main lobes:
- Anterior pituitary gland lobe (adenohypophysis) – about 70% of the gland
- Middle lobe of pituitary gland (intermediate lobe) – about 5%
- Posterior pituitary gland lobe (neurohypophysis) – about 25%
Each lobe has different pituitary gland secretions, so the pituitary gland secretes distinct sets of hormones from its anterior, middle, and posterior parts.
| Anterior pituitary gland lobe (70%) | Middle lobe of pituitary gland (5%) | Posterior pituitary gland lobe (25%) |
|---|---|---|
| Growth hormone (GH) | Melanocyte‑stimulating hormone (MSH) | Vasopressin (antidiuretic hormone, ADH) |
| Adrenocorticotrophic hormone (ACTH) | Oxytocin | |
| Luteinizing hormone (LH) | ||
| Follicle‑stimulating hormone (FSH) | ||
| Thyroid‑stimulating hormone (TSH) |
These are the major secretions of the pituitary gland that students are tested on in physiology and biochemistry examinations.
Anterior Pituitary gland lobe
The anterior pituitary is responsible for most pituitary secretions, including hormones that control growth, adrenal function, gonads, and the thyroid gland.
“Andreas Vesalius” described the pituitary body in 1543. The anterior pituitary hormones are tropic (trophikosG = nourishing) or tropins (troposG = turning) in nature, stimulating the secretion of all these hormones from target organs. Hormones secreted by the anterior pituitary are,
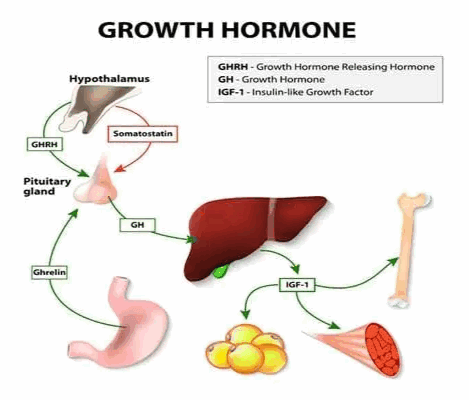
1. Growth Hormone (GH)
Chemistry:
- GH is a single polypeptide hormone with a molecular weight of about 22,000 in all mammalian species.
- GH is synthesized in somatotropes, a subclass of the most abundant cells in the anterior pituitary gland.
- It consists of 191 amino acids.
Functions:
- GH stimulates overall protein synthesis and is associated with retention of phosphorus, partly by increasing tubular reabsorption in the kidney.
- GH increases DNA and RNA synthesis, promoting cell growth.
- It increases the synthesis of collagen and other connective‑tissue proteins.
- GH brings about mild lipolysis by mobilizing fatty acids from adipose tissue via activation of hormone‑sensitive triacylglycerol lipase.
- Hypersecretion of GH can cause hyperglycemia, poor glucose tolerance, and glycosuria.
Abnormality:
- Panhypopituitarism: Decreased secretion of all anterior pituitary hormones, which may be congenital or acquired, leads to generalized endocrine failure.
- Dwarfism: Proportionate dwarfism can result from deficiency of anterior pituitary gland secretion of growth hormone during childhood.
- Levi‑Lorain dwarfism (Levi‑Lorain syndrome / Lorain‑Levi syndrome): Levi‑Lorain dwarfism is a hereditary form of pituitary dwarfism in which the pituitary secretes normal or near‑normal amounts of GH, but the liver has a reduced ability to produce somatomedin C (insulin‑like growth factor‑1, IGF‑1). This leads to short stature despite normal GH levels, and the condition is also described in the literature as Levi-Lorain syndrome, Lorain dwarfism, or Lorain-Levi syndrome, terms that students often search together.
- Acromegaly: Increased secretion of GH in adults (usually due to a pituitary adenoma) causes acromegaly, characterized by enlargement of hands, feet, jaw, and soft tissues.
For more details:
Kids and teens grow and go through puberty at different times. For girls, puberty usually begins between the ages of 8 and 13. For guys, it often begins later, between 10 and 15. You must have noticed some teens develop a lot earlier, whereas others develop much later than other people of the same age. There’s a medical reason some people grow more slowly than usual.
Reasons for slow growth:
- Genetic Reason: If you’re short, you may just have familial (genetic) short stature. Like short parents having short children.
- Lack of Nutrition: Not getting adequate amounts of protein, calories, and other nutrients in your diet can also cause growth to slow, as can some other chronic medical conditions such as kidney, heart, lung, and intestinal diseases.
- Sickle cell anemia: People with sickle cell anemia may also grow and develop more slowly. Sickle cell anemia is a blood disorder that affects hemoglobin, the protein found in red blood cells (RBC) that helps carry oxygen throughout the body. It occurs when a person inherits two abnormal genes (one from each parent) that cause their RBC to change shape.
- Constitutional growth delay: These teens grow at an average rate when they are younger kids, but they lag and don’t start their pubertal development and growth spurt until after most of their peers.
- Dwarfism results from abnormal growth of the bones and cartilage in the body. In many forms of dwarfism, the person has abnormal body proportions, such as noticeably short limbs.
- Hormones: Many diseases of the endocrine system can impact the growth of the glands that produce hormones. The endocrine glands secrete hormones that are carried throughout the body in the bloodstream. The hypothalamus (part of the brain) controls the pituitary gland, which releases some hormones that regulate growth and sexual development. Estrogen and testosterone are essential hormones that drive sexual development and function and also play a role in growth.
- Hypothyroidism: This can cause slow growth because the thyroid gland isn’t producing enough thyroid hormone responsible for proper growth.
- Turner syndrome: This is a genetic condition (because of a problem with a person’s genes) that occurs in girls. A missing or abnormal X chromosome causes it. Girls with Turner syndrome are short and rarely undergo normal sexual development because their ovaries don’t mature and function normally.
- Growth Hormone Deficiency (GHD): One growth disorder specific to the hormones that govern growth is called growth hormone deficiency. This condition involves the pituitary gland, the small gland at the base of the brain that produces growth hormone and other hormones. If the pituitary gland doesn’t produce enough hormones for healthy growth, growth slows down or stops.
Essential Facts of Growth Hormone Deficiency:
- It can occur at any age.
- The most common sign in kids and teens is a slowing of growth to less than 2 inches (5 centimeters) a year.
- Kids with this disorder usually have normal body proportions.
- Growth hormone deficiency does not affect intelligence or brain function.
- Growth hormone deficiency typically impacts only one person in a family and isn’t passed on from parents to children.
Causes:
In most cases, though, the cause of growth hormone deficiency is merely unexplained.
- Underdeveloped, damaged, or malfunctioning pituitary gland.
- Hypothalamus: This can happen before or during birth or can be caused later by an accident or trauma or certain diseases.
- Tumors near the pituitary gland, like craniopharyngioma, can also damage the hypothalamus and pituitary gland and affect growth.
Symptoms:
- Growth in Height: Affected children have an abnormally slow growth rate.
- Head: Head circumference increases typically in GHD.
- Adiposity: Because of the deficient breakdown of fats, patients have a much higher level of adipose tissue than average for their age, especially around the waist.
- Muscle: Because of reduced protein synthesis, lean body mass, reflected mainly in muscle development, is correspondingly lower than average for age.
- Genitals: Males are underdeveloped for their age, even when gonadotropin secretion is apparently normal.
- Blood Sugar Levels: Because of the inadequate breakdown of glycogen into glucose, hypoglycemia can occur, and seizures may arise if this is severe and untreated.
- Phenotypic Appearance: The above signs and symptoms lead to a “typical” phenotypic appearance for the GHD patient. Thus, patients of short stature have a chubby presence and usually a high-pitched voice. They may seem precocious because their appearance suggests a younger child, but their speech and abilities are that of an older child.
Treatment:
- Self-Care: As growth hormone deficiency can cause a lack of energy and strength, patients should eat a balanced diet, get regular exercise, and get plenty of sleep.
- Medications: The doctor may prescribe growth hormone, also called somatropin (Humatrope, Genotropin). The drug is given as a shot a few times a week that is injected underneath the fat of the patient’s skin.
- Hormone Therapy: Children and some adults with growth hormone deficiency will benefit from growth hormone therapy. The goals of treatment are to increase growth in children and restore energy, metabolism, and body composition.
Tips for the parents:
- Treat your child according to age, not size. Also, inform their teacher about the correct age.
- Encourage your child to take part in physical activities he or she enjoys.
- Increase your child’s comfort at home by making sure that essential items are within reach, such as the radio, television, stereo, and books.
- Get professional counseling for yourself and your child.
- Self-esteem reflects perceptions or feelings about oneself. Teasing and bullying can have an adverse effect on any child’s self-esteem. Keep the lines of communication open. Encourage your child to discuss any situations or circumstances that may trouble him or her.
It can be tough having a growth disorder as a teen because it can affect a person’s body image and self-esteem. Talking with a mental health professional is one way some people deal with feelings and concerns about their growth.
2. Adrenocorticotrophic hormone (ACTH)
Chemistry:
- ACTH is a straight‑chain polypeptide with a molecular weight of about 4,500.
- It comprises 39 amino acid residues in mammals such as humans, ox, sheep, and pigs.
- The most potent segment of activity lies between residues 15 and 18.
Functions:
- ACTH increases the synthesis and release of corticosteroids by the adrenal cortex.
- It promotes transfer of cholesterol from plasma lipoproteins into zona fasciculata cells of the adrenal cortex.
- ACTH induces a rise in cAMP, which activates protein kinases and stimulates cholesteryl esterase, creating a pool of free cholesterol available for steroidogenesis.
- It activates cholesterol desmolase, the rate‑limiting enzyme that converts cholesterol to pregnenolone.
- It increases the activity of dehydrogenases of the hexose monophosphate (HMP) pathway, raising NADPH needed for hydroxylation reactions.
- It activates hormone‑sensitive lipase involved in lipolysis, increasing free fatty acid levels.
Normal level:
The circulating concentration of ACTH in normal individuals is about 0.1 to 2.0 mU/dL, and the pituitary gland stores roughly 5 to 10 mg of ACTH.
Abnormality (or) Clinical importance:
Cushing’s disease:
- Over‑secretion of ACTH due to a tumor or hyperplasia of corticotrophs (β‑cells) of the anterior pituitary gland lobe leads to Cushing’s disease.
- This causes hypersecretion of glucocorticoids from the adrenal cortex.
- Clinical features include hyperglycemia, glycosuria, muscle wasting, thinning and atrophy of the skin, and increased urinary nitrogen loss.
- There is abnormal deposition of fat (e.g., moon face and truncal obesity), along with sodium and water retention and hypertension.
3. Luteinizing Hormone (LH)
Chemistry:
- LH is a glycoprotein hormone containing sialic acid, hexose, and hexosamine as the carbohydrate moiety (about 16%).
- The molecular weight of LH is about 40,000.
- LH is a dimer composed of non‑covalently linked α and β chains.
- The β chain of human LH has 112 amino acid residues.
Functions:
This hormone is also known as interstitial cell‑stimulating hormone (ICSH).
In females:
- It causes final maturation of Graafian follicles and triggers ovulation.
- It stimulates secretion of estrogen by the theca and granulosa cells.
- It supports formation and maintenance of the corpus luteum and luteinization of follicular cells.
- In the ovary, it stimulates interstitial cells to produce androgens such as androstenedione, dehydroepiandrosterone (DHEA), and testosterone.
In males, LH acts on Leydig cells of the testes to stimulate testosterone secretion.
4. Follicle‑stimulating Hormone (FSH)
Chemistry:
- The molecular weight of FSH is about 25,000.
- It is a dimer of α and β chains linked non‑covalently.
- The α chain is identical to that of LH and TSH, but the β chain of human FSH has 118 amino acid residues.
- FSH is a glycoprotein containing sialic acid, hexose, and hexosamine as the carbohydrate moiety (about 16%).
Functions:
FSH exerts its effects via specific receptors and activation of cAMP pathways.
In Females,
- It promotes growth and maturation of ovarian follicles.
- It prepares the Graafian follicle for the pre‑ovulatory LH surge.
- It enhances estrogen production in response to LH.
In Males,
- It stimulates seminiferous tubule and testicular growth.
- It plays an important role in the maturation of spermatozoa (spermatogenesis).
5. Thyroid‑Stimulating Hormone (TSH)
Chemistry:
- TSH is a glycoprotein with a molecular weight of about 30,000.
- Each molecule contains 8 to 9 cysteine residues.
- It is produced by basophil cells of the anterior pituitary gland.
- TSH consists of α and β subunits linked non‑covalently; the α subunit is nearly identical to that of LH, hCG, and FSH.
- The α subunit consists of 92 amino acids, and the β subunit consists of 112 amino acids.
Functions
TSH stimulates the thyroid gland and increases:
- Uptake of iodide from the blood by the thyroid gland
- Conversion of iodide into iodinated thyroid hormones (T3 and T4)
- Release of thyroid hormones into the circulation
These thyroid‑related pituitary gland secretions are crucial for basal metabolic rate and energy homeostasis.
Middle Lobe
The middle lobe of the pituitary gland, also called the intermediate lobe, mainly secretes melanocyte‑stimulating hormones (MSH), derived from the precursor proopiomelanocortin (POMC).
Melanocyte-stimulating Hormone (MSH)
The hormones secreted by the intermediate lobe (or middle lobe) of the pituitary gland are called “MSH.”
- POMC (proopiomelanocortin) is the precursor molecule, which is cleaved by proteases to give ACTH and β‑MSH and is related to both α‑MSH and ACTH.
- ACTH can be further cleaved to β‑MSH, which has 13 amino acids.
- α‑MSH is present in larger quantities and shares amino acids 11 to 17 of β‑MSH, which are also found in ACTH.
Functions:
MSH darkens the skin and is involved in skin pigmentation by stimulating melanocytes to deposit melanin pigment.
Abnormality:
Addison’s disease:
- Excess MSH increases melanin synthesis, resulting in diffuse brown pigmentation of the skin, a characteristic feature of Addison’s disease.
Posterior Pituitary Gland Lobe
The posterior lobe of the pituitary does not synthesize hormones but stores and releases two key pituitary secretions—vasopressin and oxytocin—that are produced in the hypothalamus and transported down the pituitary stalk.
The two major hormones are:
- Vasopressin (antidiuretic hormone, ADH)
- Oxytocin
1. Vasopressin
- Vasopressin is also called arginine vasopressin (AVP).
- If arginine is replaced by lysine, the hormone is called lysine vasopressin (LVP).
- It is a nonapeptide, consisting of nine amino acids.
Mechanism of Action:
ADH binds to membrane receptors in the kidney collecting ducts and activates adenylate cyclase. The cAMP produced activates protein kinase A, which phosphorylates proteins in microtubules and microfilaments, increasing insertion of aquaporin water channels. The net effect is increased reabsorption of water.
Functions:
- Antidiuretic effect: Vasopressin increases the permeability of collecting ducts and tubules to water, allowing most of the water to be reabsorbed as tubular fluid passes through these segments, conserving body water and producing concentrated urine.
- Urea‑retention effect: Vasopressin increases the permeability of medullary collecting ducts to urea, leading to urea retention and contributing to the hypertonicity of the renal medullary interstitium.
- Pressor effect: It stimulates contraction of vascular smooth muscle, causing vasoconstriction by increasing cytosolic Ca²⁺ concentration.
- Glycogenolytic effect: By increasing intracellular Ca²⁺ concentration in the liver, vasopressin can enhance glycogenolysis.
Abnormality:
- Deficiency of ADH leads to diabetes insipidus, characterized by excretion of large volumes of dilute urine and intense thirst.
- Excess secretion of ADH (often due to ectopic production by malignant tumors) leads to the syndrome of inappropriate secretion of ADH (SIADH), causing hypotonic expansion of extracellular fluid volume and hyponatremia.
2. Oxytocin (or) Ocytocin
The term “oxytocin” comes from the Greek “oxy” (quick) and “tokos” (birth), meaning “to stimulate birth.” Oxytocin is a nonapeptide hormone, containing nine amino acids.
Mechanism of action:
Oxytocin acts on an estrogen‑primed uterus. Near the time of labor, the number of oxytocin receptors in the uterine myometrium increases 100‑ to 200‑fold, greatly enhancing uterine sensitivity to oxytocin.
Function:
Oxytocin mainly causes smooth muscle contraction.
- Effect on uterus and birth: Oxytocin causes rhythmic contractions of the pregnant uterus, especially toward the end of gestation, and is partly responsible for the progression of labor and delivery.
- Effect on milk ejection: Oxytocin acts on the mammary gland. Suckling triggers a neuroendocrine reflex that stimulates oxytocin release, causing contraction of myoepithelial cells and expulsion of milk from the alveoli into the milk ducts.
Discover more from Biochemistry Den
Subscribe to get the latest posts sent to your email.